Goals and Objective for Inpatient Wards
- Develop an understanding of common clinical problems seen in the hospital
- PGY-1: Understand the basic principles of assessing and managing common presentations of disease in hospitalized patients
- PGY-2: Learn how to manage complex presentations of disease in hospitalized patients.
- PGY-3: Develop advanced processes to recognize and treat complications in hospitalized patients with multiple medical problems
- Competency: Patient care, Medical knowledge
- Understand the differential diagnosis of common clinical scenarios
- PGY-1: Develop a basic differential diagnosis for common clinical scenarios in hospitalized patients
- PGY-2: Develop an expanded differential diagnosis for common clinical scenarios in hospitalized patients.
- PGY-3: Recognize unusual presentations of common clinical situations in hospitalized patients.
- Competency: Medical knowledge
- Learn pharmacological management of common clinical problems.
- PGY-1: Learn the common medications utilized for the management of common clinical problems in hospitalized patients.
- PGY-2: Understand how to manage complicated clinical problems and develop specific therapeutic strategies for hospitalized patients.
- PGY-3: Learn how to develop personalized care plans for hospitalized patients with intersecting clinical problems
- Competency: Medical knowledge
- Effectively admit patients to the inpatient service, develop, and execute assessment and management plans.
- PGY-1: Learn the steps required to admit a patient and initiate admission orders. Recognize how to prioritize patient problems
- PGY-2: Develop management plans for problems identified in admitted patients
- PGY-3: Understand interactions between patient problems and develop advanced strategies to prioritize management
- Competency: Patient care
- Effectively execute day-to-day management of patients.
- PGY-1: Learn the steps required to manage patients on a daily basis including a daily assessment and determining progress in clinical problems
- PGY-2: Understand how to adjust treatment plans based on patient progress and determine the need for additional assistance such as subspecialty consultation
- PGY-3: Recognize how to manage complex medical problems and manage both expected and unexpected complications.
- Competency: Patient care
- Interdisciplinary care and discharge planning
- PGY-1: Learn how to communicate effectively with the interdisciplinary care team and anticipate patient needs for discharge and effective follow-up
- PGY-2: Recognize the unique needs of patients and help integrate patient needs with available resources
- PGY-3: Learn how to manage advanced situations such as end-of-life decisions, complex transitions of care and advocate for patients when resources are limited
- Competency: Patient care, System-based practice
- Developing diagnosis skills
- PGY-1: Learn how to effectively use bedside clinical examination
- PGY-2: Demonstrate subtle bedside clinical findings
- PGY-3: Learn how to correlate bedside clinical findings with imaging and other data
- Competency: Patient care, Medical knowledge
- Developing diagnosis skills
- PGY-1: Rational ordering of lab tests and imaging studies
- PGY-2: Learn the indications for basic laboratory investigations and imaging
- PGY-3: Learn how to interpret laboratory findings and imaging
- Competency: Practice-based learning and improvement, Medical knowledge
- Familiarity with the electronic health record and optimization of its use
- PGY-1: Develop a basic understanding of The EHR and its core components
- PGY-2: Understand and teach others on how to effectively use the electronic health record
- PGY-3: Develop an understanding of advanced medical informatics in the care of patients by utilizing additional resources in the EHR
- Competency: Systems-based practice
- Communication and teamwork
- PGY-1: Recognize the core members of the patient care team to include nurses, patient technicians, physical therapists, occupational therapists, discharge planners and hospital administration personnel
- PGY-2: Develop effective and timely communication strategies with the interdisciplinary care team
- PGY-3: Use advanced communication methods to engage and coordinate care with the interdisciplinary care team
- Competency: Professionalism, Interpersonal and communication skills
- Recognizing and responding to medical error
- PGY-1: Understand the basic principles of medical error that can result in diagnostic errors or management errors
- PGY-2: Develop an advanced understanding of preventing medical errors and recognize the role of cognitive heuristics
- PGY-3: Develop an advanced understanding of responding to medical errors, mitigating risk and communicating error to the interdisciplinary team in the patient
- Competency: Practice-based learning and improvement
- Team Structure
- Admissions
- Rounds and Staffing
- Sign-Out and Cross Cover
- Note Templates and Team Phones
- Phones & Communication
- Resources
Team Structure
Rounding Teams (Medicine A, B, and C)
- Team composition: One intern, one resident, one attending, +/- one to two medical students
- Service cap: Maximum (hard cap) 10 patients seen in one day (including new admissions and discharges)
- Admission cap: Three new admissions or transfers (must not violate service cap)
- Admitting hours: 7:00 am - 1:00 pm (Monday - Friday)
- Hours: 7:00 am - 5:00 pm (intern and resident can alternate "short" and "long" days on weekdays)
- One resident will need to stay until 7 pm on Friday and Saturday (no swing team)
- Days Off: Please note that your AmIOn will display a red moon symbol on the days you are to report to work. The dates without the red moon symbol are your days off.
Swing Team (Medicine D)
- Team composition: One intern, one resident, one attending, +/- one to two medical students
- Service cap: Swing team will admit patients from the ER or transfers from the ICU and distribute patients to the rounding teams.
- Admission cap: Four new admissions (must not violate service cap of rounding teams)
- Admitting hours 1:00 pm - 9:00 pm
- No more than 2 admissions after 7 pm
- No more than 1 admission after 8 pm
- Hours: 1:00 pm - 12:00 am (midnight), Sunday through Thursday
- Admitting attending:
- Patients admitted before 4pm – Swing attending for the day
- Day team should place MAS order in the AM switching resident and attending
- Patients admitted 4pm or later – Day attending who will inherit patient in the morning
- Co-sign H&P to corresponding day attending
- Place admission order to corresponding day attending
- Patients admitted before 4pm – Swing attending for the day
- Handoff - Team D should send handoff each night before leaving via Microsoft Teams to all residents and attendings on wards teams A, B, C, and E. Please include which team is assigned to which patient as well as pertinent information that will help the team picking up the care of the veteran in the morning. Please include Peggy "Denise" Cornett, Nicole Johnson, and Tomika Johnson in the sign out message as well. Denise and Tomika are our care coordinators and Nicole Johnson is from social work. Keeping them in the loop will expedite care and disposition for the veterans. If you having difficulty gaining access to Microsoft Teams at the VA, please reach out to Lynne Anderson () for further directions or help.
Night Float (NF)
- Team composition: One intern, will cross cover with support provided by Swing Team in the late evening and CPICU resident in early morning
- Service cap: Night float will provide cross cover on the teaching team census only
- Admission structure: Will admit with VA CPICU resident, but VA CPICU resident will remain first call on ICU patients and admissions.
- Hours: 7:00 PM - 9:00 AM

Admissions
Admitting at the VA
When should patients be admitted Observation vs. Inpatient? Why does anyone care?
- The simple answer is patient who you anticipate will be admitted < 48 hrs should be obs. Everyone else should be inpatient. If at the time of admission, you think they will stay longer than 2 days for any reason (severity of illness, evolving diagnosis, disposition/placement issues, etc), err on the side of admitting as inpatient. Example of obs appropriate admission: patients with multiple admissions of non-cardiac chest pain, typically with overnight observations and discharge who are presenting for similar complaint, very elderly people who are getting admitted for a mild COPD exacerbation but their age makes them a bit of a risk, etc.
- The VA system works a little bit differently than Parkland (PFA) or CUH (Insurance NOS). An obs encounter at the VA does not count as an admission. An admission is counted from the time you place an inpatient order. .
- Before writing delayed admission orders, please review the ADT order placed by the ED. if you disagree, cancel the old order and place a new order. When you write delayed admission orders, your ADT order stays in place and supersedes the previously placed ED ADT order, or any orders you placed prior. If you are uncertain, feel free to check with your attending and err on the side of inpatient if you’re not sure.
What is an ED Virtual Admission or Virtual Obs?
Given delays in bed availability, patients can now be admitted from the ED to a "virtual admission." This allows ED providers to sign out admission prior to a bed being ready in the hospital. The goal is to avoid the sometimes 8+ hour between when an ED provider decides to admit a patient and when a bed becomes available. Under the prior system, these patients waited (often without any orders) until they can be admitted to an internal medicine provider (either academic or hospitalist). Now, patients can be admitted without a bed assigned. This gives us the ability to take admission earlier, be more selective about teaching cases, and begin inpatient care before a patient moves to the floor.
The following flowsheet outlines the process of admitting a patient to a virtual bed from the ED.
IMPORTANT POINTS: Do not place orders until the patient's status has changed to inpatient (EDV INPATIENT) should display in the top left hand corner of the patients chart. This is handled by the ED and the MAS
- Placing orders before the conversion will result in lost orders
- Do not place your own admission order
- Placing a competing order may convert the patient's admission status and result in lost orders
- Do not place delayed orders once a patient is admitted
When patient moves to the floor, their orders should follow without delayed orders
- Discuss with nursing staff caring for patient in the ED, introduce your team as the primary
- Write a note with your team and your team phone number
- Eg: Patient admitted to Medicine Team A (Internal Medicine), Phone: xxx-xxx-xxxx. Full H/P to follow
- This will allow the nurses to contact you about urgent matters while patient remain in the ED
Orders for Patients Boarding in the ED
- New admissions are under your care after the Doc-to-Doc conversation is complete, even if they are still physically located in the ED.
- The best way to get orders carried out on your patients that are still in the ED is to ask the ED physician to order it, as the nurses rely on orders placed to physically print in the ED, and this does not happen unless you are sitting at an ED computer.
- You should check if the ED physician noted the correct resident and attending in the admit order. Also, in your delayed orders, ensure you write a "MAS text order" and specify in the free text to state the inpatient attending's name, inpatient provider's name as the resident), the team (A, B, C, or D), and team phone number to ensure communication from the nurses' and ward clerks' occurs as above.
Rounding Team (Day) Admissions
Rounding Teams (Day)
Admission time: 7:00 am to 1:00 pm
Cap: Team cap 10 patients (including admissions and discharges), admission cap: three new patients (combination of ER, transfers, swing admissions)
At the start of each shift, one resident should send an email using this template to: to let them know how many patients can be accepted by each team and what time you finish admitting. You can receive admission from the following sources:- Overnight (Swing Shift): The swing shift team will notify you of your new admissions for the morning prior to completing their shift from the day prior. The rounding teams will assume primary responsibility for these patients starting at 7:00 am (Hospital Day 1)
- ICU transfer (CPICU residents/interns): Each team may take up to one admission from the CPICU. If the CPICU calls you with an admission, please ask them to kindly call ADT first so that the appropriate flow and order of admissions is respected (and because this will allow ICU transfers to also be considered for Hospitalists and Team E). Wards teams may follow patients awaiting bed availability only if agreed upon by ICU team (including attending or fellow) and the wards resident.
- You can also contact the hospitalist group for any overnight hold overs/admits any time after 7:00 AM.
- Emergency Department: You may contact the ED CDU physician (71975) any time after 7:30 am to receive available admissions
- See attached virtural admission guide
- Direct admissions: You will be contacted directly by sources like PRIME clinic, CLC, and outpatient providers to admit patients directly
Please evenly distribute all admissions evenly amongst each admitting team on a rotating basis to ensure balanced timing of admissions. After each admission, please update the MAS order for provider and include a note with your pager number and team phone number at the top of each daily progress note.
What if my team's intern is off?
- You will be responsible for swing/overnight admissions, but NOT new daily admissions (ED etc.)
What if my team's resident is off?
- You will not be responsible for either swing shift admissions or new daily admissions
- Overnight admissions should be divided amongst teams with upper-level residents
Swing Team Admissions
Swing Admitting Team
Admission time: 1:00 pm to 9:00 pm
Cap: 4 admissions per shift (less if no wards teams have team availability)
- No more than 2 admissions after 7 pm
- No more than 1 admission after 8 pm
At the start of each shift, the senior resident should send an email using this template template to: to let them know how many patients can be accepted and what time you finish admitting.
You will admit patient from the Emergency Department and direct admissions. At the request of the ICU, transfers can be accepted in the afternoon only if mutually agreed up and deemed safe for transfer. Please notify bed control after you have reached your cap for the day.
Please include at the top of your note your team (Medicine D/Swing Admitting) and your team phone number.
Handoff: Please communicate with day team residents about the admissions you have taken in a given evening. Handoff needs to occur in Microsoft Teams. The Swing Shift Resident will be responsible for dividing the admissions amongst teams A, B, C, and E, as fairly as possible. If you having difficulty gaining access to Microsoft Teams at the VA, please reach out to Lynne Anderson () for further directions or help.
We now distribute admissions across 4 teams. The UTSW teams A, B, and C and the Baylor Team E. This means each day we will need to know how many patients each service is managing in order to keep a fair distribution cycle.
Swing attending cycle: Previously, there was a Swing Attending who you staffed with each evening, and would be on call to answer questions overnight. Starting 6/26/2022, there will not be an independent Swing Shift Attending. Currently there is a plan for Sundays and then a plan for Mondays-Thursdays.
Sundays: There is not a swing shift ;attending in house. As you admit patients, please assign them to teams, A/B/C/E. If there is a patient that is sick or has an acute issue that needs attending help, please contact the assigned/inheriting attending by phone. They have been instructed to be on-call to help with any of the admissions they will receive the following morning. Additionally, if there is a patient who you do not think should be admitted to the Resident Wards teams (usually if they are only being admitted for placement) then you can ask ADT to not admit the patient to you. The attendings are on call to support you.
Example: You don’t feel comfortable with the plan for two separate admissions. You then assign these patients to inheriting teams. Patient 1 is assigned to Team A and Patient 2 is assigned to Team B. You would call the Team A attending for help about Patient 1, and the Team B attending for help about Patient 2.
Mondays-Thursdays: You will have a swing shift attending in house for early admissions. You can call the same swing shift attending in the evening for later admissions that you have questions about. On Monday you will staff with Team A attending until roughly 4 PM. Then that night, if you feel unsafe or are unsure of the plan, you can call the Team A attending. On Tuesday, you will follow the same trend with the Team B attending, Wednesday Team C attending, and Thursday Team E attending. When you send handoff, please include the attendings in the Teams message
so they understand which patients their team will be responsible for. Your primary goal on patient distribution is fairness among teams, with a secondary goal of maintaining continuity of care by the attending.
Example: It is Monday evening. Team A is due to accept one admission on Tuesday morning. You staffed one patient with the Team A attending during the day. Please, distribute this patient to Team A such that the attending has continuity of care, instead of one of the later patients you admitted.
Regarding your H&P Cosign: If you staff an admission with an attending during the day, please cosign them to the night, otherwise cosign the admitting attending for the next day.
Attending Schedule:
VA Wards Attending Contact information
| Sunday: | A/B/C/E |
| Monday: | Team A Attending |
| Tuesday: | Team B Attending |
| Wednesday: | Team C Attending |
| Thursday: | Team E Attending |
Rounds and Staffing
Rounding Team (Day)
Rounds will begin each day at 10:00 am after morning report. Rounds should include all old patients, any new patients assumed from the swing team, and any new admission that are ready to be presented to the attending. Please discuss with your attending the best time to round on new admissions taken during the day. Please contact the chief resident at the VA for any issues surrounding rounding or rounding times. All daytime admissions must be staffed with the attending.
Care Coordination Rounds happen at 8:30 AM. Denise or Tomika (our care coordinators) will call the rounding rooms to run the list with you for the brief needs for the day. Please make every effort to be available at this time as it is critical for ensuring timely discharges.
Swing Team (Admitting Team)
Swing Team will no longer have a separate Attending. Instead, the Day Team Attendings (UTSW Team A/B/C and Baylor Team E) will rotate and staff the swing team admissions as described below:
Sundays: As the on-call resident assesses patients, they will be assigned to one of the four inheriting teams (A, B, C, or E) based on clinical volume. These patients will not be formally assessed by an attending in house on the day of admission. The patient will be staffed on Monday morning with the inheriting team and attending. If a patient is sick or there is an acute issue or question that the Swing resident needs assistance with on Sunday, please contact the respective inheriting day attending for that patient via phone. All four day attendings (teams A/B/C/E) have been instructed that they are "on-call" via phone on Sundays to help the Swing residents as needed with any of the admissions they will be receiving the following morning.
Mondays-Thursdays
- "Early" Swing Team admissions (1 PM to 4 PM) will be staffed by the pre-assigned Day Team attending after 4 PM the day of admission. These patients will stay assigned to the receiving attendings team, unless this violates the hard cap of 10 in which case the Attending will staff the admission, but the patients will need to be handed off to an uncapped team the following morning.
- "Late" Swing Team admissions (4 PM to 9 PM) will be admitted by the Swing Team residents, then distributed and handed off to the four inheriting teams the following morning. The day after admission, these patients will be staffed by the inheriting Day Team Attending as a new overnight admission. If a patient is sick or there is an acute issue/question that the Swing residents need help with overnight, they will contact the pre-assigned Day Team attending they staffed Early admissions with via phone for help.
Day Team Attending Pre-assignments
Mondays: Team A Attending
Tuesdays: Team B Attending
Wednesdays: Team C Attending
Thursdays: Team E Attending
Please discuss with your attending what time is best for staffing new admissions. All patients admitted before 4 pm should be staffed with an attending. Admissions after 4 pm will be staffed with the receiving team attending in the morning. If a patient is sick or there is an acute issue or questions that the Swing resident needs help with they will contact the inheriting Day Attending for that patient via phone.
You must hand off all patients you admit during your swing shift. VA handoff needs to occur in Microsoft Teams. A group Teams message with brief sign out on each patient you admit to each resident and intern on shift the following day should be sent, including the care coordinators and social workers as listed above. Please ensure that ALL patients are handed off before completing your nightly shift. If you having difficulty gaining access to Microsoft Teams at the VA, please reach out to Lynne Anderson () for further directions or help.
Sign-Out and Cross Cover
Rounding Team (Day)
Starting Your Day:
- Rounding teams will receive sign-out from the night float intern at 7:00 am
- Rounding teams should review evening admissions and divide overnight admissions
- All admissions admitted from the Swing Team must be distributed to the day teams evenly
- Collect your team pager and phone from the night float intern (the float team pager and phone should be held)
Finishing Your Day:
- After all daily task for the day are completed, day teams may sign out their old patients to the Swing Team (recommended 4 - 5 pm)
- Ensure that new admissions have been staffed with the attending on service for the day
- Resident an intern may alternate who is "short" and "long" on a given day, only one resident needs to sign-out to the Swing Team
- Please be respectful about cross cover tasks as you would with any other rotation
- Handoff should be thorough and complete. Handoff needs to occur in Microsoft Teams.
- Friday/Saturday: Residents must determine who will stay as "long" until 7:00 pm when the night cross cover intern arrives
- There is no Swing Shift coverage on Friday/Saturday, the night float intern will arrive at 7:00 pm to assume cross cover responsibility for the service.
Swing Team
Starting Your Day:
- You will receive sign-out (verbal and written) from the three daily rounding teams once they finish their work for a given day
- You should carry the pagers and phones for Medicine Teams A, B, C, and D
- You will be responsible for cross cover on all teaching team patients on general medicine only
- When the cross-cover resident arrives (9 pm on weekdays, 7 pm on weekends), you will hand over your cross cover responsibilities for the day
Finishing Your Day:
- Admissions that arrived before 5 pm should be staffed with your attending
- Please notify your attending of all admissions that arrive after 5 pm
- Provide handoff to the day teams who will be assuming care of your admitted patients
- We recommend a brief handoff via Microsoft Teams for each patient admitted
- VA handoff needs to occur in Microsoft Teams. On the first day of the rotation, please activate your VA Microsoft Office account. You can active your account by following these instructions: Microsoft Office Account Activation Instructions. The swing team will not be able to send sign out to individuals without an active Microsoft Office account at the VA.
- If you are having difficulty gaining access to Microsoft Teams, please reach out to Lynne Anderson (), and she will help you gain access to Teams.
- Please include the night cross cover intern and all day team rounding residents on communications
- After all patient care responsibilities have completed on new admissions, please sign-out to the night float intern (recommended 11:00 pm to 12:00 pm)
Night Float
Starting Your Day:
- Arrive at 7:00 PM
- You will receive sign-out from the Swing Team (Sunday - Thursday) or the Late Resident (Friday - Saturday) on all old patients
- After the Swing Team departs for the day, please visit the CPICU where the on call resident will assist you with any cross cover assistance and you will admit VA CPICU admissions with the on call resident.
Overnight Cross Cover:
- The night cross cover intern should carry the team pagers and phones for Medicine Teams A, B, C and D
- Night interns are strongly encouraged to work from the CPICU rounding room after the swing team departs. All management decisions involving escalation of care, major management changes, or decompensating condition, should be discussed with Swing Team resident/CPICU resident. On call resident in the CPICU will provide back up assistance and can help with orders if needed. If the CPICU resident is unavailable, the CPICU moonlighting fellow can be contacted for assistance. Please notify attending on service attending of unexpected decompensations or escalations in ICU.
- You will be expected to admit VA CPICU patients during night float
- You will be expected to present VA CPICU patients admitted overnight in the morning after signing out the floor patients to the academic teams A/B/C
- You will not be first call on any VA CPICU patients.
Finishing Your Day:
- You will sign out all cross cover events from overnight to each respective day team at 7:00 AM. Please assist in ensuring each Swing admission is assigned to a day team, and then present new VA CPICU admissions at 8:00 AM with a plan to leave by 9:00 AM.
Note Templates and Team Phones
Note Templates
The following templates can be used to efficiently document with the necessary elements. Please you the respective note heading for your team:
- Rounding Teams: Medicine A, B and C
- Swing Team: Medicine D
Please include your team and team phone # at the the top of all progress notes.
Search Function in CPRS:
Notes > “View” tab > “Search for Text”
Instructions on How to Change Your Pager Number to the Team Phone in CPRS:
When rotating on VA wards, you need to update your pager number in the VA system to be your TEAM phone (not your personal pager). Upper level residents need to do this each time they change teams. If you are a prime resident, change your pager number back to your personal pager number before you leave the VA.
- Once logged on to VA Workstation, click on GOLD STAR on desktop
- Do not start CPRS…rather go to VISTA-R2 and double click to start
- If prompted, enter in ACCESS CODE and VERIFY CODE (or your PIV card may log you in automatically)
- Once logged into VISTA, type TBOX then hit enter
- Enter ELE then hit enter
- INITIAL prompt – hit ENTER
- SIGNATURE BLOCK PRINTED NAME – hit ENTER
- SIGNATURE BLOCK TITLE – hit ENTER
- OFFICE PHONE – hit ENTER
- VOICE PAGER – hit ENTER
- DIGITAL PAGER – type in TEAM phone number. Hit ENTER.
- ENTER your CURRENT SIGNATURE CODE - just hit ENTER (no need to enter in Signature Code)
- To log out of VISTA, continue to hit ENTER 3-4 times and you will be logged off.
- To change DIGITAL PAGER back when VA rotation is done, repeat steps 1-13 typing in your personal pager number for "DIGITAL PAGER."
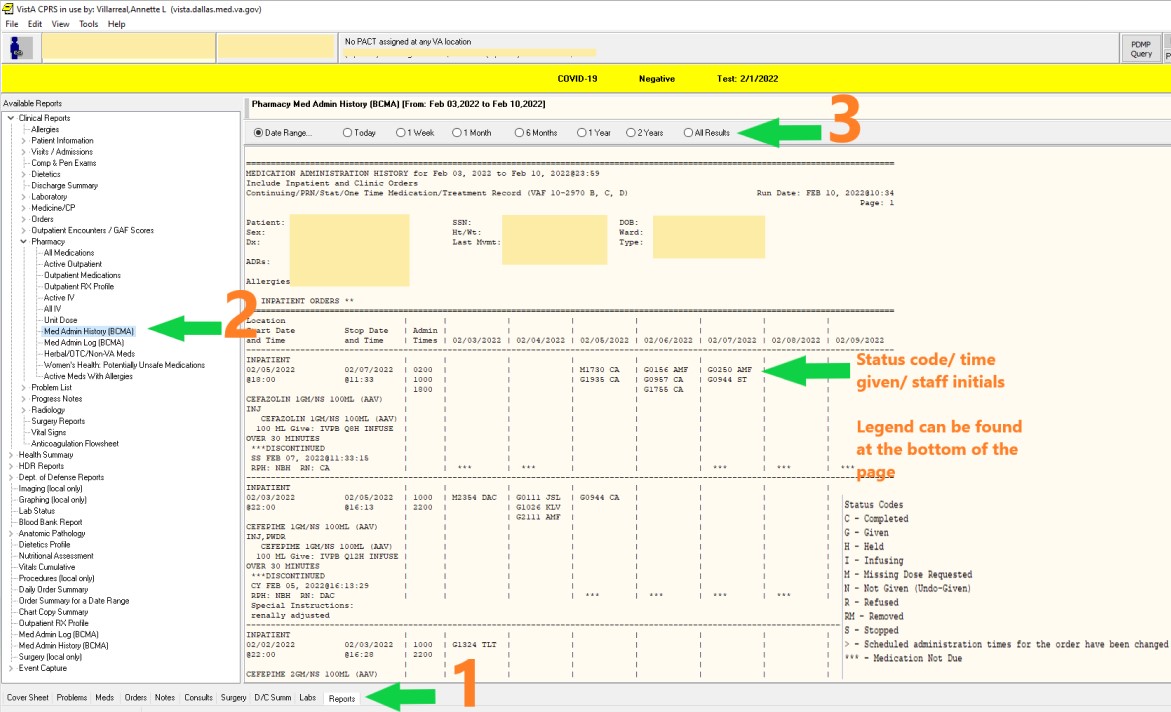
Where's the MAR ?
In CPRS
- Click on the Reports tab at the bottom of the page. Expand Clinical Reports
- Expand Pharmacy
- Select Med Admin History (BCMA
- Select date range Scroll through report. The meds are in alphabetical order.
Phones & Communication
Phones & Communication
- Each team has a Team Phone (A, B, C, D) that is carried by the intern (except for their day off, at which time it is carried by the resident). All calls from the ER, Bed Control, Nurses, and Consulting service should utilize the Team Phone, and not the residents' or interns' personal pagers. Your team phone number will be associated with your name instead of your personal pager in CPRS, so you should not receive any pages to your personal pager but you are expected to carry your personal pager in case someone outside of the VA system (including chief residents) is trying to reach you.
- Please include your Team Name and Team Phone # at the top of every daily progress note to help the nurses contact you more easily.
- To reach any of the on-call hospitalists: Can be reached 24/7 on VA issued flip phone 325-433-9937
When rotating on VA wards, you need to update your pager number in the VA system to be your TEAM phone (not your personal pager)
- Once logged on to VA Workstation, click on GOLD STAR on desktop
- Do not start CPRS…rather go to VISTA-R2 and double click to start
- If prompted, enter in ACCESS CODE and VERIFY CODE (or your PIV card may log you in automatically)
- Once logged into VISTA, type TBOX then hit enter
- Enter ELE then hit enter
- INITIAL prompt – hit ENTER
- SIGNATURE BLOCK PRINTED NAME – hit ENTER
- SIGNATURE BLOCK TITLE – hit ENTER
- OFFICE PHONE – hit ENTER
- VOICE PAGER – hit ENTER
- DIGITAL PAGER – type in TEAM phone number. Hit ENTER.
- ENTER your CURRENT SIGNATURE CODE - just hit ENTER (no need to enter in Signature Code)
- To log out of VISTA, continue to hit ENTER 3-4 times and you will be logged off.
- To change DIGITAL PAGER back when VA rotation is done, repeat steps 1-13.